CervicalCheck Update: The Scally Report
“We should have been told in 2016 when the results came in”.
Final Report anonymous contributor
Over 170 pages, 14 sections and 50 recommendations, the Scoping Inquiry into the CervicalCheck screening controversy by Dr Gabriel Scally is a comprehensive and impressive body of work. Above all, it is unquestionably patient centered. The women and families affected are given a voice by Dr Scally and positioned at the epicentre of the Irish healthcare system. Indeed, they will play an integral role in the implementation phase of Dr Scally’s recommendations into the future. We set out below the main findings of Dr Scally’s report.
Cervical screening
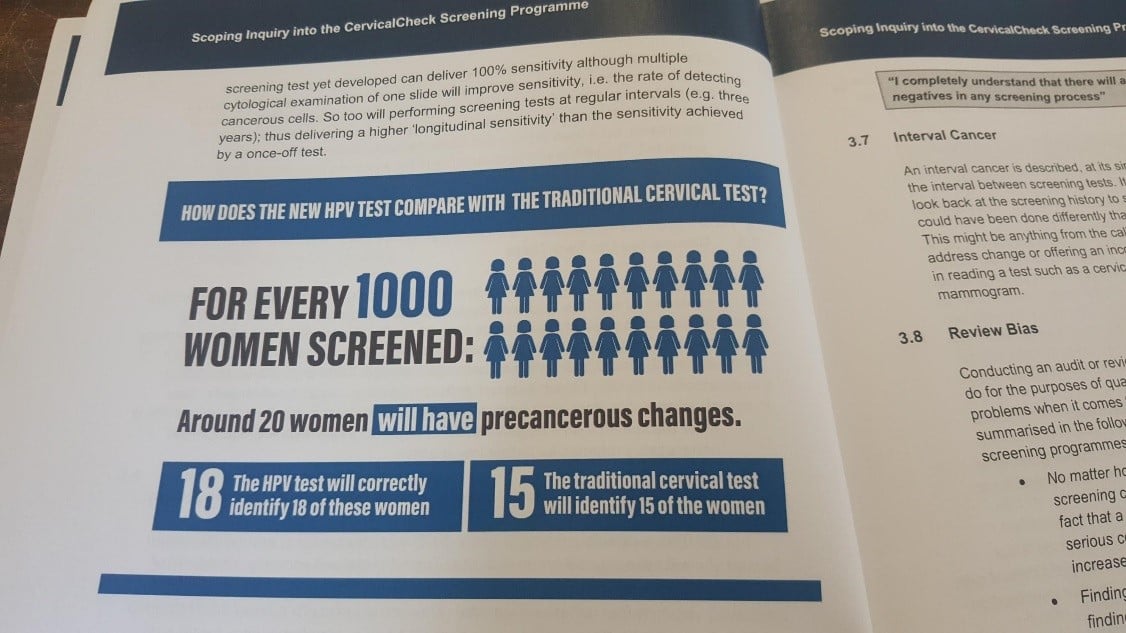
Cervical cancer is the fourth most common cancer in women worldwide with over half a million cases diagnosed every year. In Ireland there were 241 cases of cervical cancer in 2015 equating to a lifetime risk of one in every 135 women. Dr Scally found that there was “clear and undisputed evidence that properly run screening programmes offer substantial benefit to the female population of the State.” Whilst acknowledging that there is a low built in miss rate generally in medical screening programmes, Dr Scally concluded that it is vitally important that cervical screening is continued in Ireland until the new HPV testing is introduced, which will significantly increase the accuracy of screening and increase the chances of more cancers been prevented earlier.
CervicalCheck Screening Programme
In Dr Scally’s view, the CervicalCheck screening programme was “doomed to fail at some point”, and the problems he uncovered were representative of a “whole systems failure” due to a “demonstrable deficit” in governance structures.
Open Disclosure & Statutory Duty of Candour
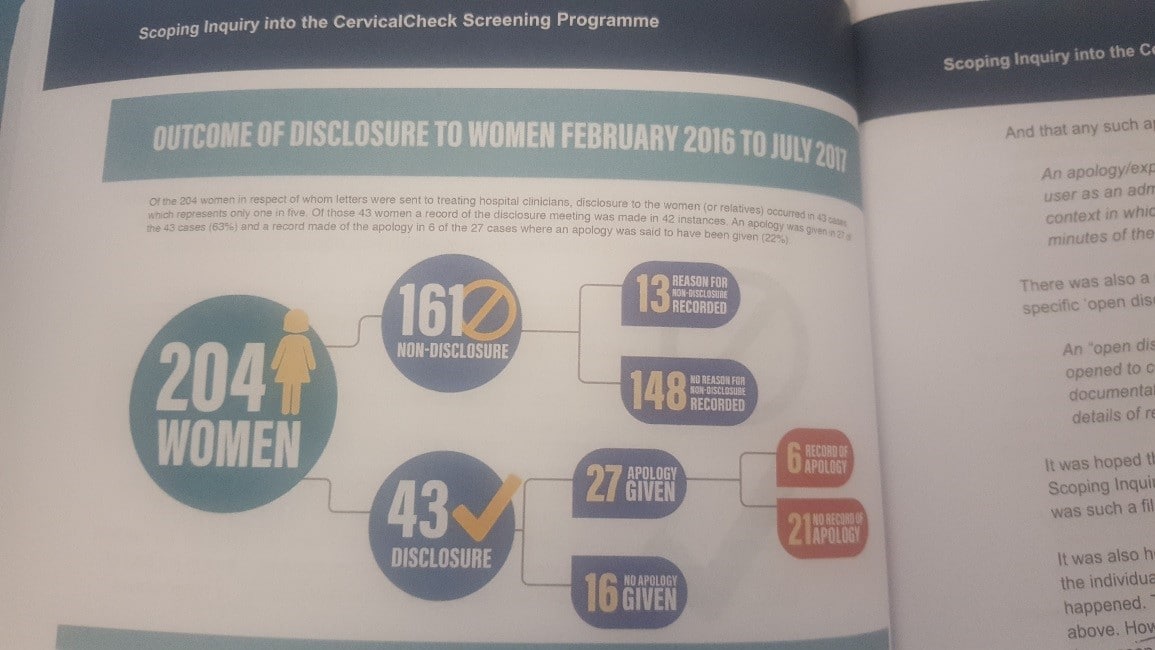
Dr Scally is scathing in his criticism of the medical profession and lamented a frustrating and prolonged discovery stage with unreasonable delays in furnishing patients’ medical records. This culture of secrecy and silence only served to “engender suspicions of obfuscation and possible cover-up.” Dr Scally found the principle of open disclosure, introduced by the HSE in 2013 and requires a hospital or healthcare provider to provide an open, consistent approach to communicating with patients and their families when things go wrong, to be “deeply contradictory and unsatisfactory”. The HSE policy guidelines combined with the Medical Council equivalent left it plain and squarely to the discretion of each medical professional to disclose or not. Of the 204 women affected by the CervicalCheck controversy, disclosures were made to women (or relatives) in just 43 cases (20%). Therefore, in 80% of cases women and their families had significant information withheld from them for several years. This statistic is a shocking indictment of the current open disclosure system in practice.
Recommendations
Dr Scally recommends that the HSE’s open disclosure policy and guidelines be revised urgently to reflect the inherent right of the patient to have full knowledge of their healthcare details including the right to know when things go wrong. This revision process is to be overseen by a working party committee with at least two patient advocates amongst its members. Exemptions to open disclosure should be limited, well-defined and subject to external scrutiny, involving a minimum of two independent patients’ advocates. An open disclosure implementation programme is to be developed to ensure open disclosure practices and policies are well understood across the health service including education and training for medical staff. A governance framework is also recommended which will include evaluation and audit. The Medical Council’s Guide to Professional Conduct and Ethics should be strengthened to ensure that doctors must promote and practice open disclosure. A statutory duty of candour for individual healthcare professionals and the healthcare organisations for which they work is recommended to bolster the concept of open disclosure which, if introduced, would be a milestone for the medical profession and the health service.
Commission of Investigation
Somewhat controversially, Dr Scally concluded that that the establishment of a Commission Investigation would be of little further benefit. Essentially, he had already uncovered the truth. Instead, he focuses on two laudable priorities: (1) the provision of maximum support to the women and families affected; and (2) the swift implementation of his 50 recommendations. A review of progress within three months of publication of the implementation plan is recommended and a further review of progress at six monthly intervals thereafter. Crucially, Dr Scally recommends the affected women and families play a prominent role in the oversight of these reviews in the future.
Conclusion
The Scally Report will not be the end. In many ways, it is just the beginning. Early implementation of his recommendations will be key. Mandatory open disclosure and a statutory duty of candour will involve a major cultural shift for Irish health professionals and the health service. They will have to embrace a culture of inquiry, one of learning from mistakes (like the airline and health and safety industries before it) to facilitate better patient outcomes in the long term.
Several other important issues remain to complete the jigsaw: mandatory reporting by hospitals of adverse medical events and near misses; Justice Meenan’s review of legal redress options for affected cancer victims (and their families), a review of the screen slides by the Royal College of Obstetricians and Gynaecology, an internal investigation by the HSE to ensure accountability where necessary, the contracting, commissioning and accreditation of cervical screening laboratories.
In the fullness of time, Dr Scally’s report may well prove to be a landmark and watershed moment for patient safety and indeed women’s health in Ireland. A full copy of the Final Report and the Terms of Reference can be found at www.scallyreview.ie